Meningitis and meningococcal epidemiology and sources of surveillance
Published on: 9th June 2025
- Surveillance
Epidemiology
Meningococcal disease
The majority of meningococcal infections occur in infants less than five years of age, with a peak incidence in those under 1 year of age. There is a smaller, secondary peak in incidence in young adults aged between 15 – 19 years of age.
Most cases of meningococcal disease occur sporadically, with less than 5% of cases occurring in clusters. Outbreaks of meningococcal disease are more common among teenagers and young adults, and outbreaks have been reported in schools and universities. Public health interventions may include vaccination (depending on serogroup) and chemoprophylaxis.
Meningococcal disease shows marked seasonal variation with a peak in winter and a low level in summer. The winter season coincides coarsely with that of influenza.
In the past 50 years, most meningococcal disease in the UK has been due to group B (MenB) and group C (MenC). The MenC vaccine introduced in 1999 has now successfully reduced cases to just a handful each year. Currently MenB accounts for the vast majority of meningococcal disease.
Meningococcal disease has a case fatality rate of approximately 10%.
Meningitis caused by other organisms
The epidemiology of meningitis due to other organisms is more complex to ascertain. Cases of meningitis resulting from infection with measles virus, mumps virus or Haemophililus influeanzae B bacteria have decreased since the introduction of routine childhood vaccination against these diseases.
After meningococcal disease, invasive infection with the bacterium Streptococcus pneumoniae (also called the pneumococcus) is one of the most frequently reported causes of bacteraemia (i.e. blood poisoning) and meningitis-see the meningococcal disease: laboratory-confirmed cases in England since 2020 to 2021 on the UK Government website (external site).
The introduction of vaccination against several pneumococcus serotypes which are particularly associated with causing invasive disease is recommended for those aged over 65, individuals in a high risk group for infection and for all children (as part of the routine childhood immunisation programme since 2006). Data on incidence of invasive pneumococcal disease, including meningitis, since the introduction of routine pneumococcus vaccination for children in the UK, is available from Public Health England.
Sources of surveillance data for Wales
Notification data
It is a statutory requirement in England, Wales, and Northern Ireland to notify all cases of clinically diagnosed meningitis, whether or not microbiologically confirmed. This statutory requirement for the notification of certain infectious diseases came into being in 1891 and includes all forms of meningitis (whatever the cause). All clinically diagnosed cases of meningococcal septicaemia must also be notified.
Whenever possible, meningitis notifications are sub categorised i.e. meningococcal, pneumococcal, Haemophilus influenzae, viral, other specified and unspecified.
The prime purpose of the notification system is speed in detecting possible outbreaks and epidemics. Accuracy of diagnosis is secondary and since 1968 clinical suspicion of a notifiable infection is all that is required. If a diagnosis of meningitis later proves incorrect it should be denotified.
With the notification system, it is difficult to accurately identify duplicate forms received from more than one physician involved in the management of the same incident case, and to completely exclude through de-notification cases wrongly diagnosed as meningitis or sub-categorised incorrectly. Therefore trends in meningitis notifications should be interpreted with caution.
Laboratory-confirmed meninogococcal disease
Over 50% of cases of meningococcal disease are ‘laboratory-confirmed’ cases. These are cases where a sample, usually of blood or spinal fluid, is taken from the sick patient and testing in a laboratory indicates the presence of meningococcal bacteria, or DNA from those bacteria. Additionally, further testing may establish which serogroup of meningococcal bacteria is responsible for disease.
However, every year there are a number of cases of meningococcal disease which are not confirmed in the laboratory. These are cases where the patient clearly has symptoms of the disease and is diagnosed on the basis of these symptoms but there is no confirmation from laboratory tests either because it is not possible to take a sample or treatment has started before a sample can be taken (which of course kills the infecting organisms).
The unconfirmed cases will not be counted in the data on laboratory-confirmed cases of disease. However, they represent a significant burden of disease.
Rates of meningitis and meningococcal disease in Wales
Number of notifications of meningococcal septicaemia, total meningitis and specified type of meningitis in Wales: 1999 to 2023
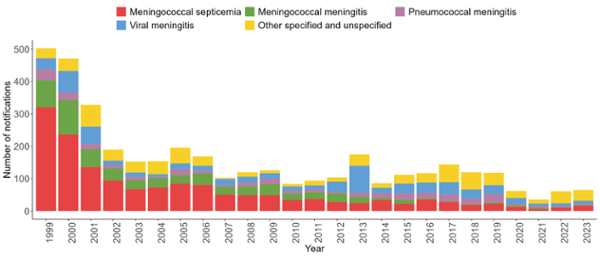
Table of contents:
- Number of notifications of meningococcal septicaemia, total meningitis and specified type of meningitis in Wales: 1999-2024
- Number of laboratory reports of Neisseria meningitidis by serogroup in Wales 2010 to 2024
- Number of laboratory reports of Neisseria meningitidis by serogroup in Wales 2010-2024
- Guidance for the public health management of meningococcal disease
- Requests for further surveillance data
- Links to other meningitis/meningococcal surveillance
- Related reports
- Related data
Caveat: Meningococcal notifications are only available up to 05/07/2024.
Number of notifications of meningococcal septicaemia, total meningitis and specified type of meningitis in Wales: 1999-2024
| Year | Notifications of menigococcal septicaemia | Total notifications of menigitis | Meningococcal notifications of meningitis | Pneumococcal notifications of meningitis | Haemophilus influenzae notifications of meningitis | Viral notifications of meningitis | Other specified notifications of meningitis | Unspecified notifications of meningitis |
| 1999 | 321 | 182 | 83 | 34 | 6 | 34 | 13 | 12 |
| 2000 | 237 | 234 | 106 | 23 | 4 | 67 | 16 | 18 |
| 2001 | 136 | 192 | 55 | 16 | 8 | 54 | 22 | 37 |
| 2002 | 94 | 96 | 38 | 10 | 3 | 14 | 17 | 14 |
| 2003 | 68 | 85 | 28 | 9 | 3 | 14 | 10 | 21 |
| 2004 | 73 | 81 | 29 | 4 | 1 | 8 | 21 | 18 |
| 2005 | 85 | 110 | 26 | 18 | 2 | 18 | 25 | 21 |
| 2006 | 81 | 88 | 35 | 9 | 7 | 15 | 13 | 9 |
| 2007 | 51 | 52 | 24 | 5 | 0 | 19 | 4 | 0 |
| 2008 | 49 | 71 | 27 | 12 | 1 | 18 | 8 | 5 |
| 2009 | 49 | 77 | 34 | 17 | 1 | 17 | 7 | 1 |
| 2010 | 34 | 50 | 20 | 9 | 0 | 13 | 7 | 1 |
| 2011 | 37 | 57 | 21 | 9 | 3 | 12 | 3 | 9 |
| 2012 | 28 | 76 | 26 | 5 | 5 | 32 | 7 | 1 |
| 2013 | 25 | 150 | 18 | 13 | 6 | 84 | 11 | 18 |
| 2014 | 34 | 52 | 6 | 15 | 1 | 17 | 3 | 10 |
| 2015 | 22 | 90 | 13 | 19 | 1 | 31 | 2 | 24 |
| 2016 | 36 | 81 | 3 | 17 | 2 | 32 | 6 | 21 |
| 2017 | 28 | 116 | 2 | 21 | 0 | 38 | 3 | 52 |
| 2018 | 19 | 101 | 2 | 17 | 2 | 29 | 10 | 41 |
| 2019 | 22 | 96 | 4 | 26 | 1 | 28 | 1 | 36 |
| 2020 | 13 | 49 | 4 | 5 | 1 | 18 | 0 | 21 |
| 2021 | 6 | 30 | 4 | 5 | 0 | 8 | 0 | 13 |
| 2022 | 11 | 50 | 0 | 3 | 0 | 10 | 6 | 31 |
| 2023 | 16 | 49 | 2 | 5 | 0 | 9 | 0 | 33 |
| 2024 | 19 | 21 | 0 | 2 | 0 | 5 | 1 | 13 |
Caveat: Meningococcal notifications are only available up to 05/07/2024.
Number of laboratory reports of Neisseria meningitidis by serogroup in Wales 2010 to 2024
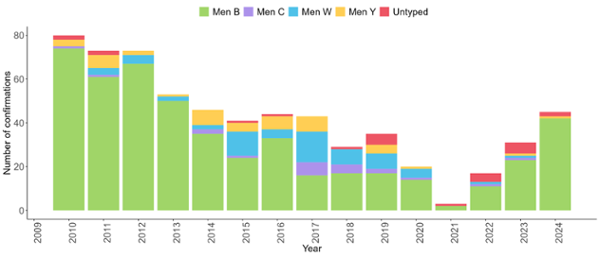
Source: reconciled data from Public Health Wales IBID laboratory confirmed cases and the Public Health England Meningococcal Reference Unit
Number of laboratory reports of Neisseria meningitidis by serogroup in Wales 2010-2024
| Year | Group B | Group C | Group W | Group Y | Not available | Total |
| 2010 | 74 | 1 | 0 | 3 | 2 | 80 |
| 2011 | 61 | 1 | 3 | 6 | 2 | 73 |
| 2012 | 67 | 0 | 4 | 2 | 0 | 73 |
| 2013 | 50 | 0 | 2 | 1 | 0 | 53 |
| 2014 | 35 | 2 | 2 | 7 | 0 | 46 |
| 2015 | 24 | 1 | 11 | 4 | 1 | 41 |
| 2016 | 33 | 0 | 4 | 6 | 1 | 44 |
| 2017 | 16 | 6 | 14 | 7 | 0 | 43 |
| 2018 | 17 | 4 | 7 | 0 | 1 | 29 |
| 2019 | 17 | 2 | 7 | 4 | 4 | 35 |
| 2020 | 14 | 1 | 4 | 1 | 0 | 20 |
| 2021 | 2 | 0 | 0 | 0 | 1 | 3 |
| 2022 | 11 | 1 | 1 | 0 | 4 | 17 |
| 2023 | 23 | 1 | 1 | 1 | 5 | 31 |
| 2024 | 42 | 0 | 0 | 1 | 2 | 45 |
Source: reconciled data from Public Health Wales IBID laboratory confirmed cases and the Public Health England Meningococcal Reference Unit
Guidance for the public health management of meningococcal disease
This is available from the Public Health England website (external site).
Requests for further surveillance data
If further surveillance data for meningitis and meningococcal disease in Wales are required, it may be possible to provide them on special request using the surveillance data request form (external site).
Links to other meningitis/meningococcal surveillance
- Public Health England (external site).
- Health Protection Scotland (external site).
- Health Protection Surveillance Centre Ireland (external site).
- Centers for Disease Control and Prevention (CDC)-USA (external site).
Related reports
-
Rapid response on deaths of children from meningitis and meningococcal disease
Background This rapid response on deaths of children from meningitis and meningococcal disease in Wales is undertaken for, and at the request of, Welsh Government. It seeks to describe the […]
Published on: 1st October 2014